
SUMMARY and EXPLANATION: Vasculitis and Acute Renal Failure following Cv19 Vaccination
Several cases of post-Cv19-vaccination vasculitis with renal failure have now been published; physicians and policy-makers should be attentive to this pattern and should report observed cases

Pattern: Several cases of post-Cv19-vaccination vasculitis with renal failure have now been published; physicians and healthcare policy-makers should be attentive to this pattern and report observed cases to Vaccine Adverse Event Reporting System (VAERS) in the United States or the local reporting system in other countries
Biological plausibility: Most vasculitic diseases associated with renal failure are mediated by immune complexes (chains of antibodies and antigens, described below) which is entirely consistent with the medical-political (mis)use of vaccines which are advertised to provide “protective antibodies”, despite the major biomedical faults of this argument, which seems to gain acceptance only among people with a limited (and therefore exploitable) understanding of Immunology.
Antigen = a molecule which triggers the formation of antibodies; hence, antigen is simply an abbreviation of antibody-generating; here, let’s represent an antigen with the symbol 0, which you can consider to be a virus or a bacteria or other antigen
Antibody = a Y-shaped protein with two heads that bind to two antigens and the tail/base that functions as a receptor (attachment site) for immune cells; here, let’s represent an antibody with the symbol Y; an antibody could bind to one antigen as 0Y or to two antigens as 0Y0 or a single microorganism displaying multiple antigens can be attacked by numerous antibodies such as 0YYYYYYYYY.
Immune complex = chains of antibodies and antigens, here symbolized as 0Y0Y0Y0Y0Y0Y0Y0Y0Y…
Immune complex disease = chains of antibody and antigens get lodged in narrow vessels (vasculitis) especially in the lungs, kidneys, skin and joints, leading to local inflammation and tissue damage
Vaccines are therefore expected to trigger immune complex diseases such as vasculitis, at least occasionally, as noted in these examples
"Vaccination (notably influenza) is a recognized trigger for the relapse of idiopathic NS [nephrotic syndrome] and ANCA-associated vasculitis. Acute onset of MCD has been reported at 4 and 18 days following the influenza vaccine and 6 weeks following a tetanus–diphtheria–poliomyelitis vaccination." Nephrol Dial Transplant. 2021 Jul 10.1093/ndt/gfab215
First description of immune complex vasculitis after COVID-19 vaccination with BNT162b2. BMC Infectious Diseases 2021 Sep 10.1186/s12879-021-06655-x
Reactivation of IgA vasculitis after COVID-19 vaccination. Lancet Rheumatology 2021 Jul 10.1016/S2665-9913(21)00211-3
Cv19 Vaccination is purported to trigger formation of so-called “protective antibodies” (Y) which are supposed to bind to the antigen (0) of the spike protein, produced endogenously via the mRNA vaccines. This is expected to produce immune complexes (0Y0Y0Y0Y). Thus the provocation of immune-complex-mediated disease such as vasculitis with acute renal failure is entirely predictable, indeed expected to occur in some patients.
Safety measures overridden: The new Cv19 vaccines were allowed to bypass normal and expected safety testing in order to achieve “emergency authorization” for a condition with fatality rate of less than 1% buttressed by falsified diagnostic criteria, inaccurate testing that grossly overestimated the number of “cases”, and falsified death-attribution criteria that allowed persons killed by firearms, persons killed in traffic accidents, deceased terminally-ill persons in hospice to be included within Cv19 death statistics to inflate the numbers; not only are these vaccines unproven to have justifiable risk-benefit ratios but the use of new mRNA technology is also completely novel, untested, and unproven prior to the rushed Emergency Use Authorization (EUA), which has now been in place for an unprecedented and inexcusable amount of time.
According to the US CDC, 37% of healthcare providers have acknowledged witnessing a *recognized* adverse vaccine event but only 17% have made a report to VAERS.
Therefore, 55% of healthcare providers have remained silent by failing to file a VAERS report even after witnessing one or more adverse vaccine reactions.
Post-marketing surveillance: The United States uses a pathetically weak passive reporting system which is generally described as receiving only 1-10% of actual vaccine injuries; internationally, doctors are untrained in recognizing adverse vaccine events, discouraged from making reports, and even when these events are noted by medical staff, the medical staff commonly fail to formally report such events. According to the US CDC, 37% of healthcare providers have acknowledged witnessing a *recognized* adverse vaccine event but only 17% have made a report to VAERS. 55% of healthcare providers have remained silent even after witnessing one or more adverse vaccine reactions. Clinicians should receive paid-protected time for filing these reports and thereby helping to safeguard patient care, industry integrity, and medical professionalism; the fact that clinicians do not receive paid-protected time for filing adverse drug effect (ADE) reports shows that the “medical system” of education, hospital training, medical organizations (etc) does not want these reports to be filed, even for the sake of patient protection and professional integrity.

Risk-to-benefit ratio: The absolute risk reduction (ARR) for the Cv19 vaccines is remarkably low; the ARR calculated by the frauded over-optimistic numbers provided by the drug companies (ie, not verified by independent researchers) is approximately 1% so the risk-to-benefit ratio in the real world is unlikely to be favorable.
Research fraud and misconduct: per Covid-19 Researcher blows the whistle on data integrity issues in Pfizer’s vaccine trial. BMJ 2021 Nov;375:n2635 10.1136/bmj.n2635
Lack of timely follow-up of patients who experienced adverse events
Protocol deviations not being reported
Vaccines not being stored at proper temperatures
Mislabeled laboratory specimens, and
Targeting of research staff for reporting these types of problems.
Previous evidence of harm: Vaccines are well-known to trigger/exacerbate a wide range of inflammatory and autoimmune disorders (some of which are specifically mediated by immune complexes), as I have noted in the following table which I extracted from Journal of Autoimmunity 2013:

Previous evidence of fraud: The drug company Pfizer is famous for fraud and has been found guilty several times for falsifying data and for misleading physicians and politicians.
"In the largest health care fraud settlement in history, pharmaceutical giant Pfizer must pay $2.3 billion to resolve criminal and civil allegations that the company illegally promoted uses of four of its drugs, including the painkiller Bextra, the U.S. Department of Justice announced Wednesday. Rubin R. Pfizer fined $2.3 billion for illegal marketing in off-label drug case. USA TODAY 2009 Sep abcnews.go.com
"American pharmaceutical giant Pfizer Inc. and its subsidiary Pharmacia & Upjohn Company Inc. (hereinafter together "Pfizer") have agreed to pay $2.3 billion, the largest health care fraud settlement in the history of the Department of Justice, to resolve criminal and civil liability arising from the illegal promotion of certain pharmaceutical products, the Justice Department announced today." Justice Department Announces Largest Health Care Fraud Settlement in Its History (September 2, 2009) justice.gov
Summary: Several cases of post-Cv19-vaccination vasculitis with renal failure have now been published; physicians and policy-makers should be attentive to this pattern and should report observed cases to Vaccine Adverse Event Reporting System (VAERS) in the United States or the local reporting system in other countries.
Citations:
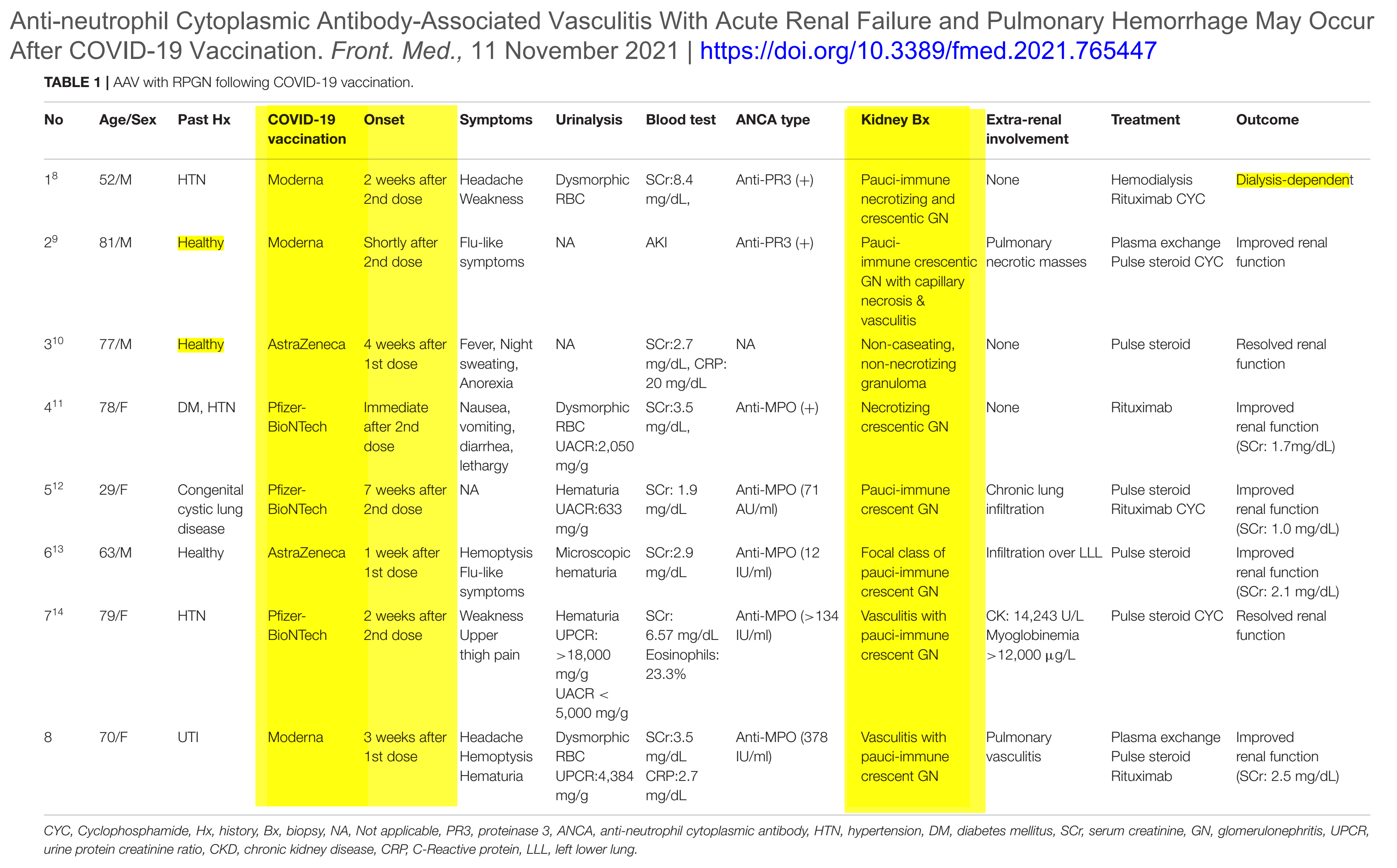
Anti-neutrophil Cytoplasmic Antibody-Associated Vasculitis With Acute Renal Failure and Pulmonary Hemorrhage May Occur After COVID-19 Vaccination. Frontiers in Medicine 2021 Nov 10.3389/fmed.2021.765447
First description of immune complex vasculitis after COVID-19 vaccination with BNT162b2. BMC Infectious Diseases 2021 Sep 10.1186/s12879-021-06655-x
Reactivation of IgA vasculitis after COVID-19 vaccination. Lancet Rheumatology 2021 Jul 10.1016/S2665-9913(21)00211-3
Covid-19 Researcher blows the whistle on data integrity issues in Pfizer’s vaccine trial. BMJ 2021 Nov;375:n2635 10.1136/bmj.n2635
"Vaccination (notably influenza) is a recognized trigger for the relapse of idiopathic NS [nephrotic syndrome] and ANCA-associated vasculitis. Acute onset of MCD has been reported at 4 and 18 days following the influenza vaccine and 6 weeks following a tetanus–diphtheria–poliomyelitis vaccination." Nephrol Dial Transplant. 2021 Jul 10.1093/ndt/gfab215
