


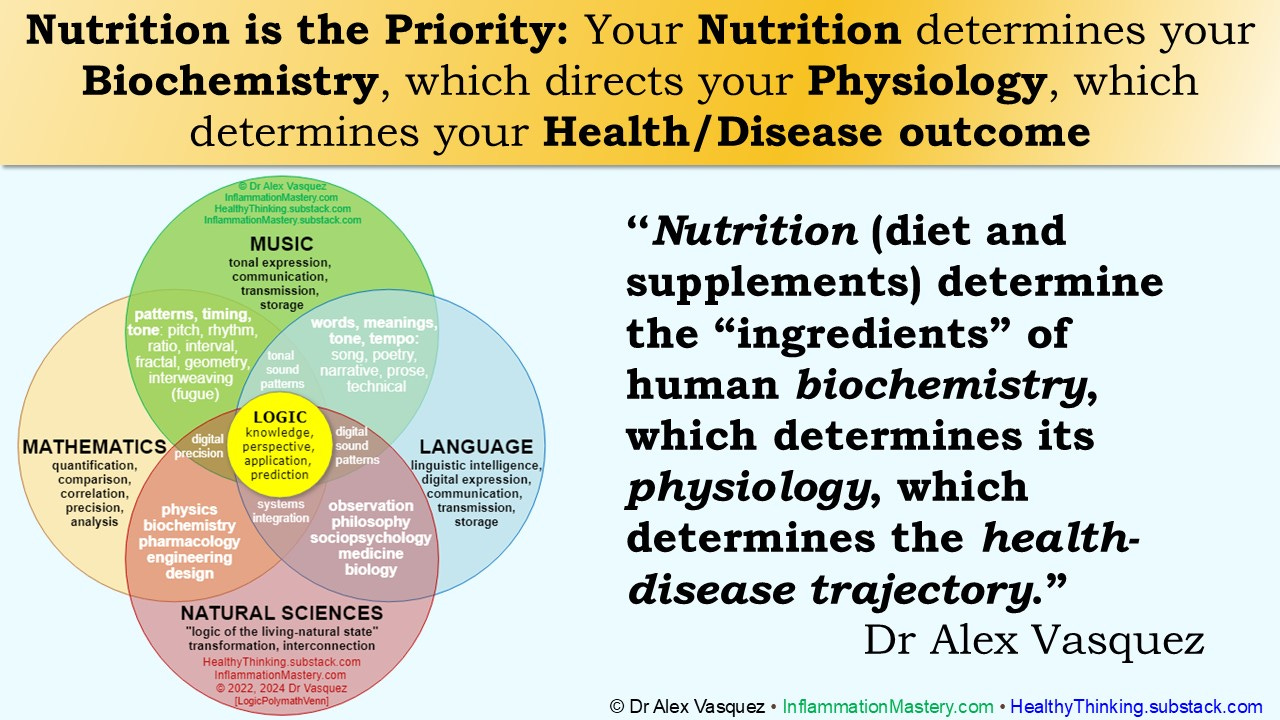
Your Nutrition determines your Biochemistry, which directs your Physiology, which determines your Health/Disease outcome
“Nutrition (diet and supplements) determine the “ingredients” of human biochemistry, which determines its physiology, which determines the health-disease trajectory.” Dr Alex Vasquez

“Nutrition (diet and supplements) determine the “ingredients” of human biochemistry, which determines its physiology, which determines the health-disease trajectory.” Dr Alex Vasquez
As I said before (May 2022 [part1] and again on May 2022 [part2]), and hopefully you’ve heard from other sources in your life as well:
We all have to stretch and exercise our mental abilities if we are to maintain them and grow them.
Read something difficult/challenging every day, even if only for a few minutes.
Here is a single paragraph that I wrote and re-wrote yesterday, introducing the topic of so-called “essential fatty acids.” Turned out that this was a good reminder for me on the topic of fatty acids.
This one paragraph contains nearly everything you need to know about fatty acids, fish oil, etc. I invite you to take a read of it, even if some of the terms and concepts are new to you.
Human physiology requires the external provision and dietary intake of fats/oils that contain the subcomponents of fatty acids in the omega-3 class and the omega-6 class, which are so categorized based on the location of an unsaturated carbon-carbon bond (ie, C=C) when counted from the methyl/omega (”n”) end of the hydrocarbon chain; this apparently minor structural detail in biochemistry translates into huge differences in the physiologic effects of n3 versus n6 fatty acids and is therefore of clinical importance. Because the prehistoric/preindustrial diet of humans contained ~7 grams per day of omega-3 (n3) fatty acids (n3FA) and thus human physiology became dependent on this regular provision, in today’s setting of a relative/absolute deficiency of n3FA (<1 gram per day), we commonly find clinical benefit of n3FA supplementation, such as with flax seed oil providing n3 alpha-linolenic acid (ALA) and more powerfully with fish oil providing the biologically potent n3 eicosapentaenoic acid (EPA) and n3 docosahexaenoic acid (DHA). Given that n3FA are generally anti-inflammatory (as well as cardioprotective, anti-diabetic, and anti-cancer) and that omega-6 fatty acids (n6FA) are generally pro-inflammation/cancer/diabetes/psychopathy, the modern misanthropic shifting the absolute and relative amounts of these fatty acids in the human diet by reducing n3FA and increasing n6FA has changed the previous ratio of 1:1 or 1:2 to the current ratio of ~1:25 and has greatly (albeit almost invisibly) contributed to the increased prevalences of inflammatory, malignant (cancer), metabolic (diabetes) and mental diseases.[1] We can accurately generalize that the n3 fatty acids ALA, EPA, and DHA are anti-inflammatory and health-promoting via various mechanisms (eg, cell membrane function, prostaglandin formation/balance, gene expression), and that these anti-inflammatory benefits are clinically important, commonly at the same levels of effectiveness as pharmaceutical drugs yet with greater safety, better affordability, and numerous collateral benefits. The n6 fatty acids linoleic acid (LA, from seed/grain/corn oil) and arachidonic acid (ArA) are clearly pro-inflammatory in addition to promoting cancer/tumor growth, disordered metabolism, and altered gene expression, promoting a diseased phenotype. As such, a commonly employed anti-inflammatory strategy by nutrition-knowledgeable clinicians is that of reducing n6 intake via dietary modification while increasing n3 intake via supplementation. The exception to the rule that “n6 fatty acids are pro-inflammatory” is that of gamma-linolenic acid (GLA, and its active metabolite dihomo- gamma-linolenic acid [DGLA]), which is both anti-inflammatory and anticancer/antitumor. GLA is an intermediate metabolite between LA and ArA and is prevented from conversion to ArA by the provision of EPA and DHA from fish oil; more precisely, one of the enzymes (delta-5-desaturase) that converts GLA to ArA is inhibited by EPA and DHA from fish oil. Because of the valuable clinical benefits of fatty acid (FA) supplementation and the need to supplement with each of the most important anti-inflammatory fatty acids—ALA, EPA, DHA, GLA, and oleic acid from olive oil—for optimal clinical benefit, I have described this approach as “CFAT—combination fatty acid therapy”, outlined in several published papers[2], chapter 4 of Inflammation Mastery, and a video presentation originally recorded for my graduate students; the articles and videos are available at HealthyThinking.substack.com/p/dr-vasquezs-cfat-combination-fatty
[1] Simopoulos AP. Essential fatty acids in health and chronic disease. Am J Clin Nutr. 1999 Sep;70(3 Suppl):560S-569S. This is a famous, classic, landmark paper.
[2] Vasquez A. Reducing Pain and Inflammation Naturally: Part 1—New Insights into Fatty Acid Biochemistry and the Influence of Diet. Nutritional Perspectives 2004 Oct. Vasquez A. Reducing Pain and Inflammation Naturally: Part 2—New Insights into Fatty Acid Supplementation and Its Effect on Eicosanoid Production and Genetic Expression. Nutritional Perspectives 2005 Jan. Vasquez A, Pizzorno J. Concerns About the Integrity of The Scientific Research Process-Focus on Recent Negative Publications Regarding Nutrition, Multivitamins, Fish Oil and Cardiovascular Disease. Integr Med (Encinitas). 2019 Feb;18(1):8-15. PMID: 31341427; PMCID: PMC6601430.
Dr Vasquez's CFAT: Combination Fatty Acid Therapy [ARCHIVED VIDEO]
![Dr Vasquez's CFAT: Combination Fatty Acid Therapy [ARCHIVED VIDEO]](https://substackcdn.com/image/fetch/w_1300,h_650,c_fill,f_webp,q_auto:good,fl_progressive:steep,g_auto/https%3A%2F%2Fsubstack-video.s3.amazonaws.com%2Fvideo_upload%2Fpost%2F152592568%2Ff98ac8f7-4e2c-4591-bc8e-491aed77a720%2Ftranscoded-00001.png)
As this platform has evolved to allow embedded/posted/included videos, some of the previously shared videos are being archived directly into the the website. FYI—be sure to see today’s post on newer research on the use of fatty acids in the treatment of chronic headache
Health Homework (3.1) FEED yourself some BRAIN CANDY [books, audiobooks]
![Health Homework (3.1) FEED yourself some BRAIN CANDY [books, audiobooks]](https://substackcdn.com/image/fetch/w_1300,h_650,c_fill,f_webp,q_auto:good,fl_progressive:steep,g_auto/https%3A%2F%2Fbucketeer-e05bbc84-baa3-437e-9518-adb32be77984.s3.amazonaws.com%2Fpublic%2Fimages%2F2d7c66f8-579f-44f3-a9ea-32700c4796fe_324x500.jpeg)
Bonus: This article includes 2 complete PDF books
Health Homework (3.2) GIFT yourself this BRAIN CANDY VIDEO: War on Sense-making, Schmachtenberger 2019
Sloppy thinking, fake $cience, and psychological manipulation (not diseases and viruses) are the biggest threats to human survival, health, happiness, and freedom.