Microbiome and Dysbiosis Video #4: My Most Nonlinear Discussion on Technological PseudoCertainty vs Effective Empiricism
While most of my written and presented work is intentionally linear, this particular conversation was more fluid—actually, during most of the time spent on this video, I was picturing lava lamps

This page was updated February2025 to include the video directly embedded (not streaming from another host) for better reliability/viewability. The video is available/viewable at the bottom of this page directly from the substack platform.
Microbiome & Dysbiosis Video #4: Clinical Approach: Testing Microbes vs Treating Dysbiosis
While most of my written and presented work is intentionally linear, this particular conversation was a bit more fluid—actually, most of the time that I was preparing-recording-editing-reviewing this video, I was picturing lava lamps in the background.

Lava lamp photo by Dean Hochman,CC BY 2.0, commons.wikimedia.org/w/index.php?curid=79022567
In medicine and healthcare education, we are mostly taught to confirm each diagnosis before preceding to treatment, and generally this is appropriate. However, when dealing with complex and subtle multicomponent functional disorders, I argue that this approach is at least occasionally if not commonly impractical, myopic, and unsuccessful.
In post-graduate education such as conferences, most of the presenters who discuss “assessment” will focus on laboratory testing either by unconscious default, laziness or inability to tackle the problem abstractly, or because they are sponsored by laboratory companies that sell testing kits and results for assessment of microbiome and other components of dysbiosis. As such most conversations on treating dysbiosis include an excess of emphasis on laboratory testing.
Treating dysbiosis differs from treating an acute infection
Dysbiosis is chronic, whereas acute infections are characteristically short-lived.
Dysbiosis is nearly always polymicrobial, whereas acute infections are more commonly monomicrobial.
Dysbiosis always has numerous predispositions and perpetuating factors, whereas infections might have only one predisposing factor.
Dysbiosis nearly always has a component of systemic or metastatic inflammation, whereas with acute infections the inflammation is mostly local.
Acute infections are more easily and justifiably treated with drug antibiotics, whereas dysbiosis requires multicomponent treatment for long durations.
Dysbiosis nearly always has primary or secondary nutritional deficiencies, which may or may not occur with acute infections.
Acute infections are typically localized whereas dysbiosis can occur in multiple locations due to multiple microbes at the same time—I was the first to describe this as multifocal polydysbiosis.
The more complex the illness (eg, autoimmunity) the more likely is multifocal polydysbiosis.
Using laboratory assessment for each aspect of multifocal polydysbiosis is impractical or impossible; much of the data comes from research investigations that have used sophisticated laboratory/biopsy interventions that are impossible or impractical to replicate in clinical practice—we use that data to inform empirical treatment without being slaves to laboratory confirmation.
Reminders and refreshments:
This video is viewable only on the website at this page (use browser) for Dysbiosis video no4, even though the text is visible via email and in the app
This video is available to, for, and by the supporting/paid subscribers who have shown enthusiastic interest in these topics
See the Course Index for the complete list of videos and related books and articles
Adjustments for volume, rewind, and full-screen mode are within the video frame; if needed, see additional instructions on how to watch videos here
Video #4 (1 hour and 18 minutes) Clinical Approach: Testing Microbes vs Treating Dysbiosis
This video is viewable only on the website at this page (use browser) for Dysbiosis video no4, even though the text is visible via email and in the app
Thank you for supporting this effort and buying me a coffee while I work in exchange for the years, weeks, and hours invested in preparing, recording, and editing this video.
Subscribe now for immediate access
Peer-reviewed (independently published) articles related to this material provided by Dr Vasquez:
Nutritional and Botanical Treatments Against Silent Infections and Gastrointestinal Dysbiosis Commonly Overlooked Causes of Neuromusculoskeletal Inflammation and Chronic Health Problems. Nutritional Perspectives 2006 academia.edu/39481031
Mitochondrial Medicine Arrives to Prime Time in Clinical Care: Nutritional Biochemistry and Mitochondrial Hyperpermeability ("Leaky Mitochondria") Meet Disease Pathogenesis and Clinical Interventions. Integr Med (Encinitas) 2014 Aug;13(4):44-9 pubmed.ncbi.nlm.nih.gov/26770108
Reply to "role of Western diet in inflammatory autoimmune diseases" by Manzel et al. In current allergy and asthma reports (volume 14, issue 1, January 2014). Curr Allergy Asthma Rep2014 Aug;14(8):454. doi: 10.1007/s11882-014-0454-4 pubmed.ncbi.nlm.nih.gov/24947682
Neuroinflammation in fibromyalgia and CRPS is multifactorial. Nat Rev Rheumatol 2016 Apr;12(4):242. doi: 10.1038/nrrheum.2016.25 pubmed.ncbi.nlm.nih.gov/26935282
Biological plausibility of the gut-brain axis in autism. Ann N Y Acad Sci 2017 Nov;1408(1):5-6. doi: 10.1111/nyas.13516 pubmed.ncbi.nlm.nih.gov/29090837
Correspondence regarding Cutshall, Bergstrom, Kalish's "Evaluation of a functional medicine approach to treating fatigue, stress, and digestive issues in women" in Complement Ther Clin Pract 2016 May. Complement Ther Clin Pract 2018 May;31:332-333. doi: 10.1016/j.ctcp.2016.10.001 pubmed.ncbi.nlm.nih.gov/27814977
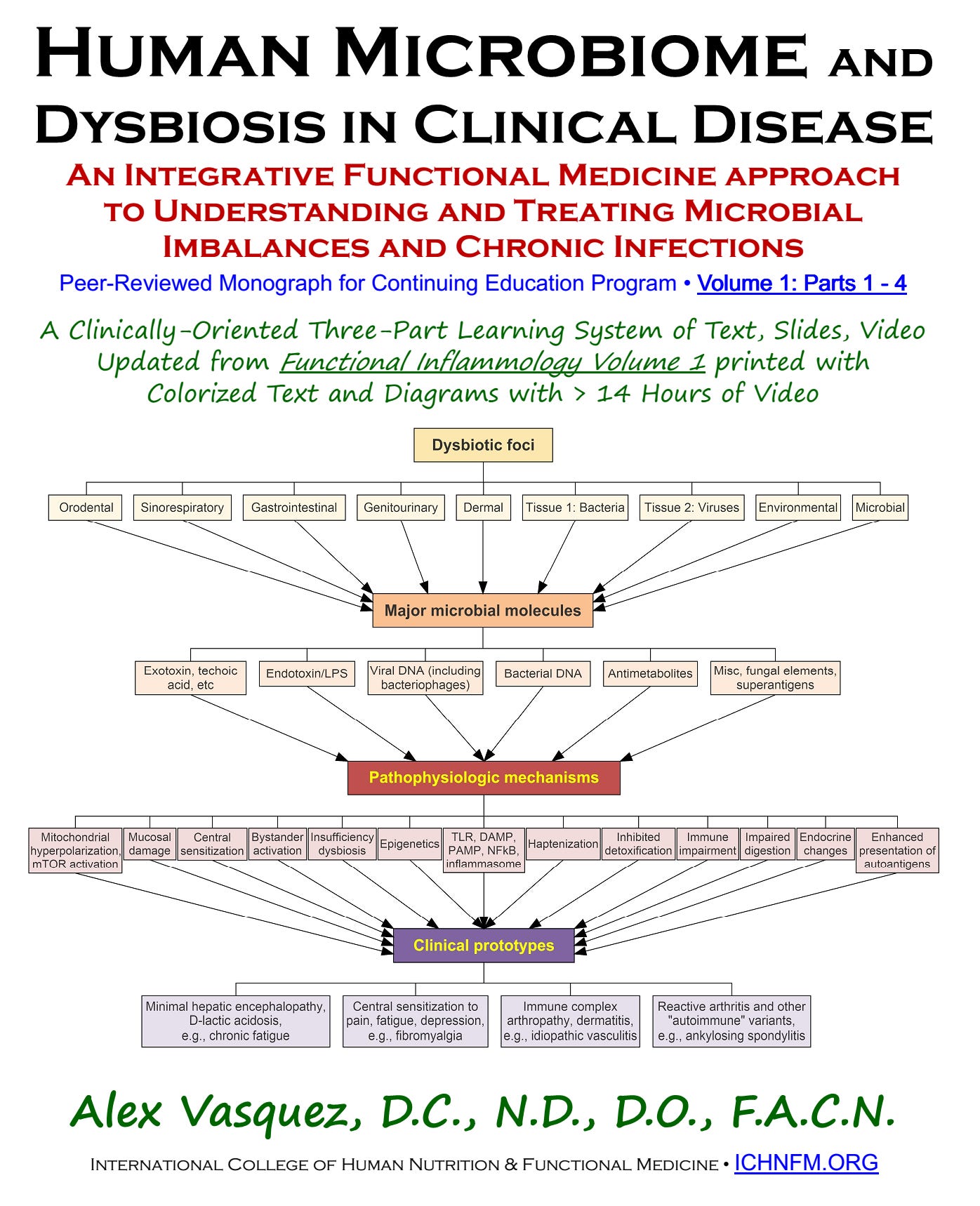
Dr Alex Kennerly Vasquez (introduction; brief Bio-CV) writes and teaches for an international audience on various topics ranging from leadership to nutrition to functional inflammology. Major books include Inflammation Mastery, 4th Edition (full-color printing, 1182 pages, equivalent to 25 typical books [averaging 60,000 words each]), which was also published in two separate volumes as Textbook of Clinical Nutrition and Functional Medicine (Volume 1: Chapters 1-4; Volume 2: Chapter 5—Clinical Protocols for Diabetes, Hypertension, Migraine, Fibromyalgia, Rheumatoid Arthritis, Psoriasis, Vasculitis, Dermatomyositis and most other major inflammatory/autoimmune disorders); several sections have been excerpted including Antiviral Strategies and Immune Nutrition (ISBN 1502894890) (aka, Antiviral Nutrition [available as PDF download] and Brain Inflammation in Chronic Pain, Migraine, and Fibromyalgia. Dr Vasquez’s books are available internationally via bookstores such as BookDepository, Amazon.com, Barnes and Noble, ThriftBooks, AbeBooks, BetterWorldBooks, WaterStonesBooks and his new Telegram channel is https://t.me/DrAlexVasquez.

Listing of Videos Currently Available
Update 2025: All videos are being re-uploaded in Feb-May 2025 to provide direct and reliable access through the substack platform:
Microbiome Dysbiosis (1) Course Overview and Introduction to Major Concepts and Mechanisms
Microbiome Dysbiosis (3) Prototypes of Dysbiosis-Induced Disease (VIDEO:1hour,42minutes=102minutes)
Microbiome Dysbiosis (7) Dysbiosis by Location—Genitourinary Tract
Microbiome Dysbiosis (8) Dysbiosis by Location—Blood, Tissue, Parenchymal Dysbioses
Microbiome Dysbiosis (9) Dysbiosis by Location—Skin and Environmental Dysbiosis
MICROBIOME DYSBIOSIS (10) Gut Dysbiosis Prototypes and Solutions, part1, part2, part3, part4, part5
MICROBIOME DYSBIOSIS (11a) GUT-BRAIN AXIS and OPTIMAL DIET, Part 1 of 2 parts covering everything you need to know